Healthy skin protects our body against various microorganisms. The basic element of this protection is the epidermis, especially the stratum corneum and the lipid coat on its surface. Additional defence against pathogenic microorganisms is provided by specific and non-specific immune mechanisms. Also, the acid reaction on the skin surface (pH 5.4 - 5.9) favours relatively less harmful bacteria and protects against pathogenic strains.
Ecthyma
This is a purulent dermatitis with ulceration usually caused by group A β -haemolytic streptococcus and staphylococcus aureus. It occurs more frequently in children and immunocompromised patients, as well as in cases of poor hygiene. Infection occurs through the penetration of micro-organisms through injury sites.
Initially, a vesiculo-purulent lesion appears on an erythematous base, and then the infection penetrates more deeply, damaging the dermis and causing a scab-covered ulceration. The lesions are most commonly located on the lower limbs, as well as the trunk and buttocks. They are usually accompanied by lymphadenitis and lymphadenopathy.
Non-arthritis should be differentiated from leg ulcers of different aetiologies: leucoclocal vasculitis, sclerosing erythema, pyoderma gangrenosum.
General treatment with an antibiotic, usually penicillinase-resistant pen icillin or cephalosporin, and local disinfectant treatment is used.
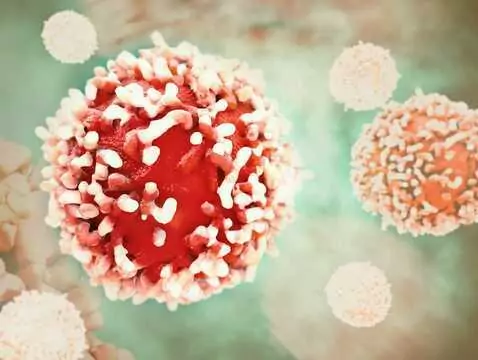
 Staphylococcal and streptococcal infection, photo: panthermedia
Staphylococcal and streptococcal infection, photo: panthermedia
Inflammation of the subcutaneous tissue(cellulitis)
This is an infection of the skin and soft tissues, often also involving fascia, muscles and tendons, caused by group A β -haemolytic streptococci or staphylococcus aureus. In most cases, infection occurs through bacterial entry into the skin through micro-injuries, surgical wounds or colonisation of the skin in patients with sepsis. Lesions are most commonly localised to the lower limb. The first symptoms are erythema and swelling, but not as clearly demarcated as in rosacea. They are accompanied by soreness and restricted mobility of the joint concerned. Lymphadenitis, lymphadenopathy and septicaemia may develop.
Inflammation of the subcutaneous tissue should be differentiated above all from deep vein inflammation and rosacea.
For limited lesions in a generally healthy person, oral antibiotics, mainly penicillin or cephalosporins, are usually sufficient. In patients with general symptoms, parenteral administration of antibiotics is usually necessary.
Chronicpyoderma vegetans et exulcerans
Chronic ulcerative skin infection with papillary lesions at the wound edges. The cause may be an infection with various bacteria, primarily streptococci, S. aureus and Enterobacteriaceae .
The lesion, usually single, 3 to 10 cm in size, occurs mainly on the limbs, buttocks and groin. It has the character of an inflammatory focus with nodules around the periphery and ulceration or necrosis or fistula in the central part. It gradually enlarges. Papillary growths may be present within the lesion.
Deep fungal infections, tuberculosis, pyoderma gangrenosum should be considered in the differential diagnosis.
Systemic antibiotics are indicated, often for up to several weeks. Sometimes it is necessary to include short-term glucocorticosteroid therapy to reduce inflammation.
Bacterial eczema - diagnosis
Inflammatory-ulcerative lesions of mixed streptococcal and staphylococcal aetiology located in the skin folds, axillae, underarms, intertriginous and submammary folds. Contributing factors include; excessive sweating, obesity, diabetes mellitus, hygiene neglect.
Yeast dermatitis, tinea capitis and erythematous dandruff should be considered in the diagnosis.
As a rule, local treatment with antibiotics, usually mupirocin, is sufficient.